Part I: OTC
Common encounters
P -> GSL switches
RECLASSIFICATIONS
- Amorolfine
- Minoxidil (female hair loss)
- Benzoyl peroxide 5% w/v
Common encounters
Eczema (dermatitis)

SIGNS and SYMPTOMS
- Don’t jump to conclusions!!
- Is this an ongoing inflammatory condition or as a result of an irritant?
- …and if so, remove the irritant!!
- Itching (…obviously!!!)
- Vague, poorly defined borders… comes and goes…
- Treatment failure!
- Lesions on face (think disfigurement!)
- Widespread or severe
- …and of course signs of infection!
- Bacterial: Crusting skin? (oozing, yellow/green)
- Viral: Blisters and bubbles (colourless weeping)
- Fungal: Flaking/circular lesions?
TREATMENT GOAL – Hydrate/reduce inflammation
- Emollients, liberally (n.b. sensitizing)
- Hydrocortisone (1% w/v), BD 7d, age >10
- Clobetasone (0.05% w/v), BD 7d, age >12
- Although Rutter suggests that these medicines can be used in pregnancy please refer to the eMC:

- With these agents do not apply to cracked or broken skin
- Do not supply if patient is taking oral steroids
- 45m window between application of both agents!!
Headlice

SIGNS and SYMPTOMS
- As before… don’t jump to conclusions!
- Beware of possible tricks i.e. sighting of shells or itching.
- The only definitive diagnosis of headlice is direct visual confirmation!!
Rule out seborrheic dermatitis!

Cradle cap
Effectively treated with coconut or olive oils!

(Malassezia spp.)
…and dandruff (pityriasiscapitis)!!

In these cases TREATMENT with:
- Coal tar
- Zinc pyrithione
- Ketoconazole
N.B. leave in hair for a few minutes before washing off
TREATMENT GOAL – Removal!
- Dimeticone.
- Dimeticone.
- Dimeticone…
- Treat covering whole head of hair and leave on overnight for 8h. Wash off in morning. Treat again after two weeks (this is imperative as dimeticone only kills live lice).
- Do not be tricked into using anything else. This is the only product with any evidence.
- Essentially it suffocates the (live) louse… and lice can’t develop resistance to suffocation.
Psoriasis

SIGNS and SYMPTOMS
- Areas of inflamed skin with scaly skin.
- This can help differentiate vs. eczema
- Commonly found on elbows, knees, forehead and less often on back
Psoriasis on arm, Marnanel (2004)
Acne
- Treatment failure!
- Widespread or severe (e.g. Cysts or nodules)
- Rosacea? Perioral dermatitis?
- …and of course signs of infection!
- Bacterial: Crusting skin? (oozing, yellow/green)
- Viral: Blisters and bubbles (colourless weeping)
- Fungal: Flaking/circular lesions?

TREATMENT GOAL
- Prevent scarring
- Benzoyl peroxide (2.5/5/10% w/v), BD
- Nicotinamide, BD
- Side-effects are generally drying of skin, reduce dose to OD in this instance.
Scabies

SIGNS and SYMPTOMS
- Difficult to precisely diagnose.
- Features very similar to eczema or psoriasis.
- Commonly found in finger webs, under arms and other body crevices.
- Intense itching.
- Widespread or severe
- …and of course signs of infection!
- Bacterial: Crusting skin? (oozing, yellow/green)
- Viral: Blisters and bubbles (colourless weeping)
- Fungal: Flaking/circular lesions?
TREATMENT GOAL
- Removal
- Premethrin (>12), full tube (sometimes more), leave on overnight!
- Malathion (>6 months)
- Repeat treatment after 7 days.
- Treat everywhere from neck down. A missed area might provide a safe place for the parasite to breed.
Fungal infections

Tinea curis – Found in groin area


SIGNS and SYMPTOMS
- Circular, flaky skin.
- Dermatophyte, named as per its location on the body.
- Can cause itching.
Fungal infections
- Treatment failure!
- Lesions on face (think disfigurement!)
- Widespread or severe
- …and of course signs of infection!
- Bacterial: Crusting skin? (oozing, yellow/green)
- Viral: Blisters and bubbles (colourless weeping)
- Fungal: Flaking/circular lesions?
TREATMENT GOAL – Removal
- Ketoconazole, clotrimazole (1%!!!), miconazole.
- All ages
- Continue treatment for up to one week after clearance of lesion.
- Terbenafine (>16)
SPECIAL MENTION…

- Note: in this image >2 nails affected = referral.
- Treated with amorolfine 5% w/v
- Takes 6 months to clear!
- >18s
- File and clean before application!
- Diabetes, pregnancy or treatment failure
Tinea unguium

•Diabetes, pregnancy or treatment failure
Warts, Veruccas and Corns



SIGNS and SYMPTOMS
Best diagnosed visually
- Treatment failure!
- Lesions on face (think disfigurement!)
- Widespread or severe
- Diabetics/immunocompromised patients
- Corns causing pain when walking (best reviewed by GP or podiatrist)
- …and of course signs of infection!
TREATMENT GOAL – Removal

- Silver nitrate pencil
- Salicylic acid (Salactol®)
- Clever marketing might suggest that more Salicylic acid will mean better efficacy… This is not the case!
- All products show similar efficacy!
- Interestingly these products have no lower age limit
- N.B. the much sought after ‘cryotherapy’ is no more effective than salicylic acid in wart removal!
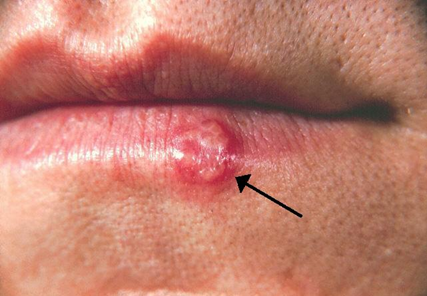
Coldsores (Herpes Simplex 1, HSV1)
*Genital lesions caused by HSV2

- Treat with Aciclovir 5%, 5 times daily. 5d.
- Care for repeated visits!
- Diabetics/immunocompromised patients
- Lesions >14d.
- Severe or widespread
- Secondary infection!!
- Can spread to eye!!
Sun and the skin
- Various grades and appearances! (SCC, BCC and MM)
- Beware of complacency!
- Can mimic other conditions!
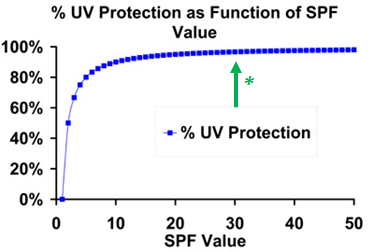
- Best treatment is prevention
- Suncream >SPF 30.
- Stay out of mid-day sun
- (10:00-14:00)

A: Asymmetrical?
B: Border jagged?
C: Various colours?
D: Diameter? Larger than a pencil rubber (6 mm)?
E: Evolving… is this lesion different or changing?
- New lesion in patient >60?
- Immunocompromised?
N.B. Chemical based sun creams penetrate the skin with unknown systemic consequences. I err on the side of barrier preparations


Miscellaneous
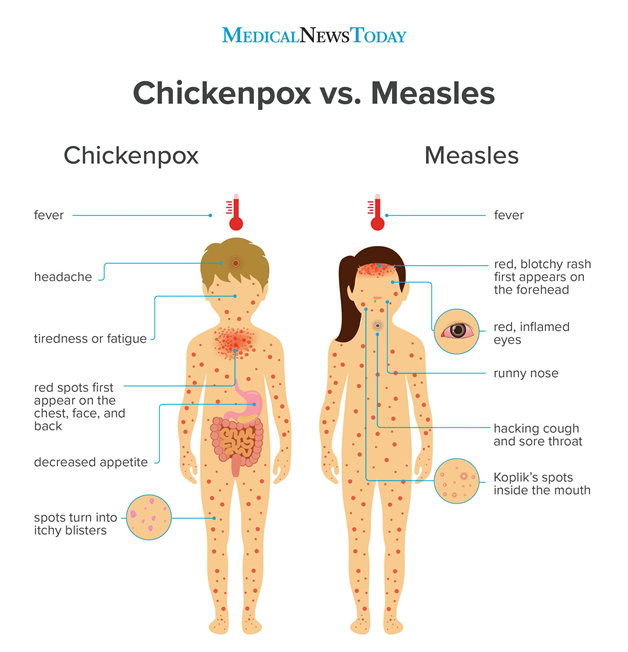
- Note that rash is generally LAST SIGN of measles!
- Measles on the rise due to anti-vax movement
- Chicken pox (varicella zoster virus)
- Can lead to shingles in later life.
- Treatment re: calamine lotion or zinc oxide creams
- Paracetamol and antihistamines OK
- Generally lasts a week.
- Keep nails short!!
- Finger-tip unit!
- One FTU should cover x2 adult hands/one arm/face or half a leg!
- Search skin conditions on reputable medical websites
- This will increase your likelihood of recognizing them (and their various facets) in the exam, and more importantly in real life!!
- Many skin products have preservatives/agents that can cause dermatitis!!!
- As far as I’m aware the only product that has none is Doublebase®
- Why leave a 45 min gap between topical applications?
- You will essentially make an extemporaneous product on the patient’s skin! Diluting the concentration of the therapeutic agents and therefore their activity!